Dilation & Curettage (D&C)
A comprehensive guide to Dilation & Curettage (D&C) — clinical indications, procedure types, recovery milestones, risks, insurance coverage, and costs in India.
Dilation & Curettage (D&C)
A comprehensive guide to Dilation & Curettage (D&C) — clinical indications, procedure types, recovery milestones, risks, insurance coverage, and costs in India.
Medically Reviewed ByDr. N V Gowthami MullangiLast updated: 16 July 2026Free Second Opinion
Get connected with a trusted doctor for an expert second opinion through our care team—at no cost.
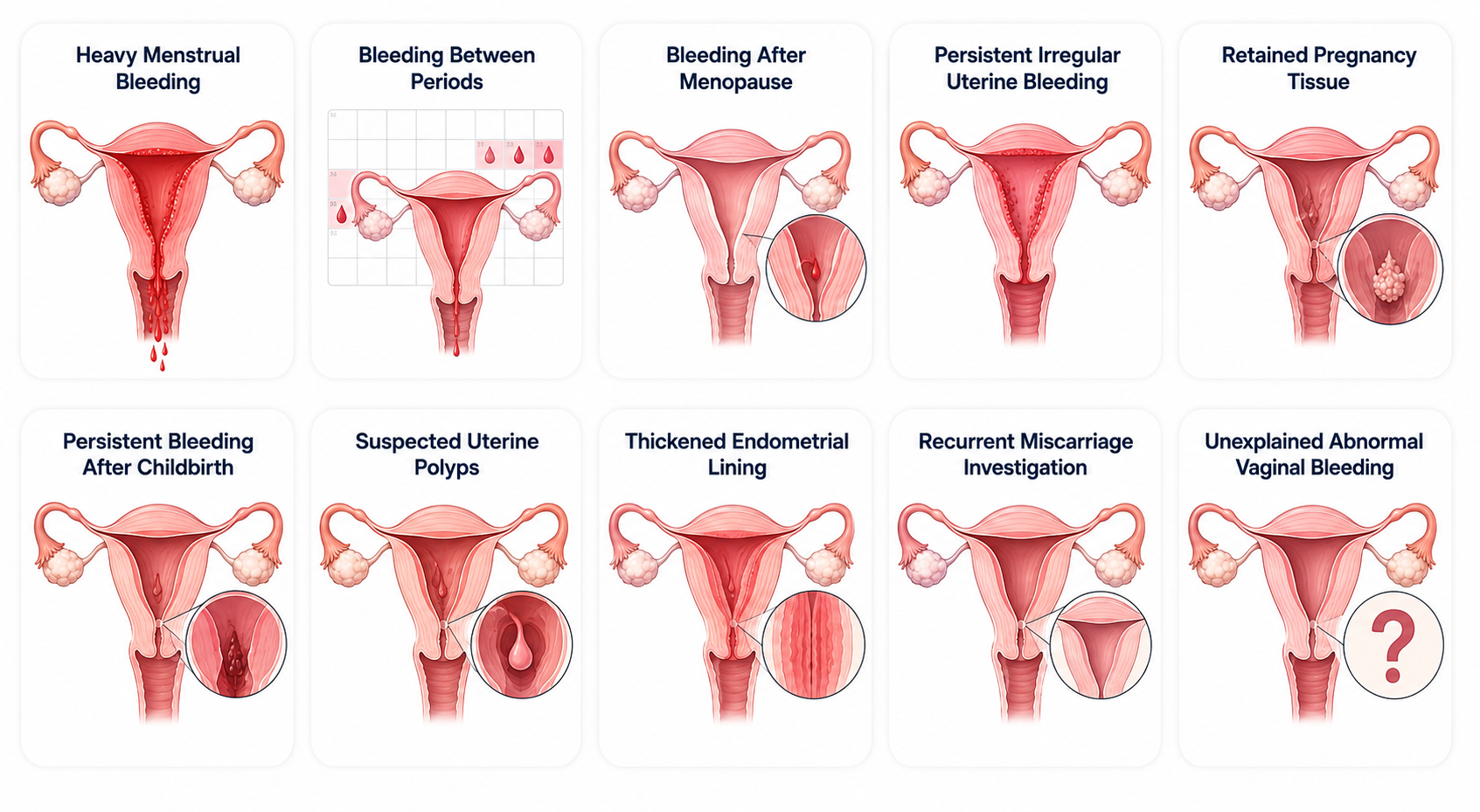
Clinical Indications for a D&C Procedure
A D&C procedure may be recommended when a patient experiences acute, unresolved gynecological symptoms that point toward an underlying intrauterine issue:
1. Abnormal Uterine Bleeding Patterns
- Menorrhagia, heavy menstrual bleeding that disrupts regular daily routines
- Intermenstrual bleeding, unexpected bleeding or tracking occurring actively between periods
- Postmenopausal bleeding, fresh or recurring vaginal bleeding occurring months or years after menopause
- Intractable cycles, irregular uterine bleeding patterns that do not show clinical improvement with standard oral medicines
- Unexplained hemorrhaging, unexplained abnormal vaginal bleeding requiring emergency diagnostic evaluation
2. Post-Pregnancy Indicators
- Retained pregnancy tissue, products of conception that fail to pass naturally following a miscarriage event
- Postpartum hemorrhage, persistent, heavy bleeding after childbirth driven by structural fragments left attached inside the uterus
3. Structural & Diagnostic Finding Markers
- Uterine polyps, suspected benign growths anchoring to the endometrium wall that prompt cyclical spotting
- Lining thickening, an abnormally thickened uterine lining visualized directly on a baseline pelvic ultrasound scan
- Recurrent early loss, recurrent miscarriages requiring localized cellular investigation to check lining receptivity
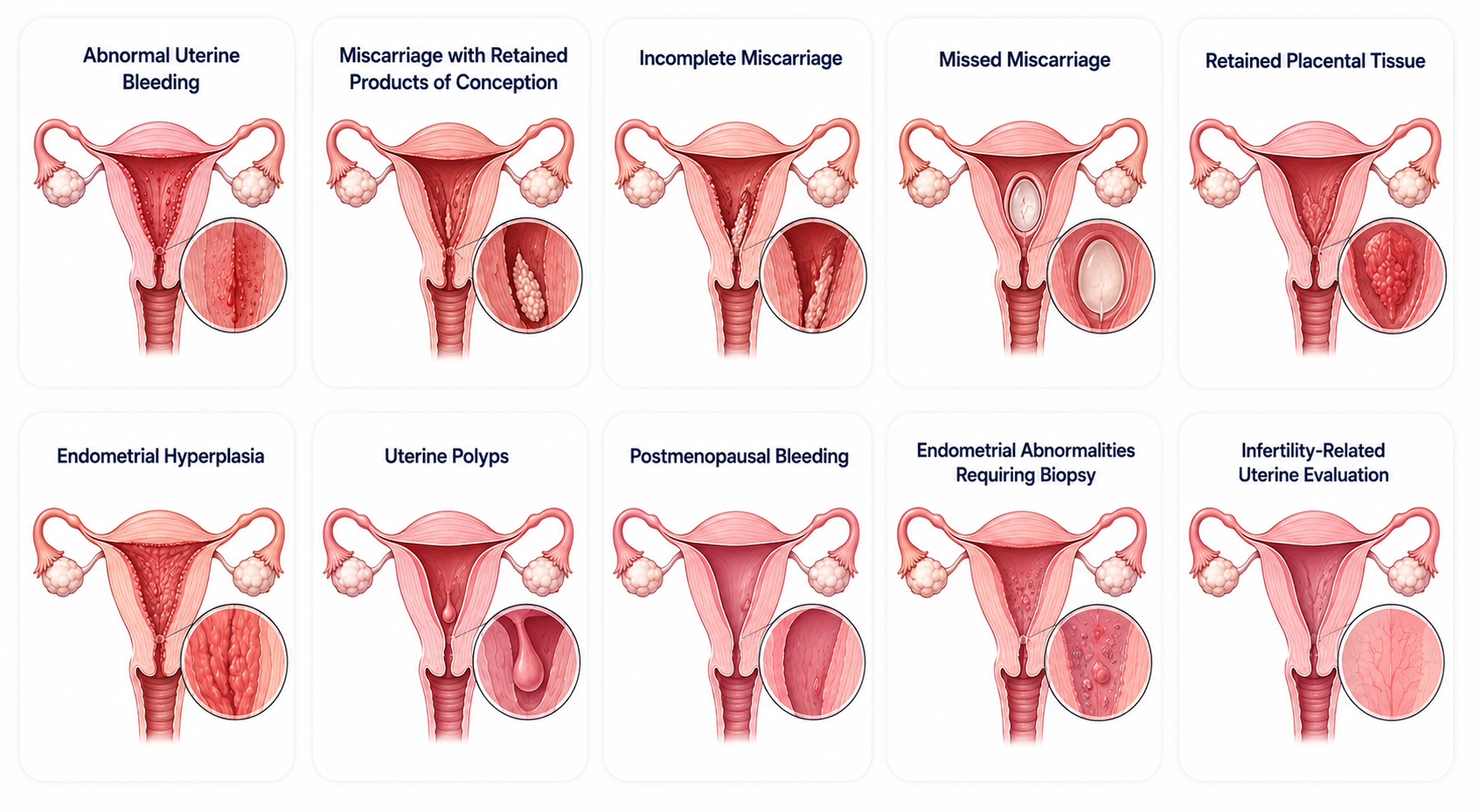
Common Conditions Treated
1. Non-Cancerous & Obstetric Conditions
- Abnormal uterine bleeding, unregulated or chronic bleeding patterns needing immediate diagnostic and therapeutic resetting
- Retained products of conception, a complication where tissue remains inside the cavity following an incomplete miscarriage
- Missed abortion management, clearing the womb safely during a missed miscarriage scenario when the body stalls natural tracking
- Retained placenta, obstetric management to remove stubborn retained placental tissue strings after baby delivery
- Uterine polyps, benign growths localized on the endometrial wall layer that cause cycle disruptions
2. Hyperplastic & Staging Conditions
- Endometrial hyperplasia, abnormal thick overgrowth of tissue cells requiring clearance and path checks to rule out atypia
- Postmenopausal bleeding anomalies, evaluating unexpected bleeding phases to safely cross-check for cell mutations
- Endometrial abnormalities, suspicious focal findings requiring specialized operative biopsy or formal testing extraction
- Infertility barriers, evaluation of structural endometrial conditions preventing proper embryonic attachment
What Causes These Intrauterine Conditions?
The need for a diagnostic or therapeutic D&C typically arises when underlying physiological changes or obstetric complications affect the natural shedding cycle of the uterine lining:
- Anovulatory cycles, irregular ovulation patterns that cause an imbalance between estrogen and progesterone, leading to an over-thickened lining that bleeds unpredictably
- Arrested miscarriage resolution, a biological delay where the uterine muscles fail to fully expel non-viable placental or embryonic tissue blocks naturally
- Abnormal tissue proliferation, localized cellular overgrowths driven by systemic hormonal surges that manifest as endometrial polyps or hyperplastic cell sheets
- Placental adherence, a condition where microscopic fragments of the placenta remain firmly anchored to the uterine wall bed after childbirth
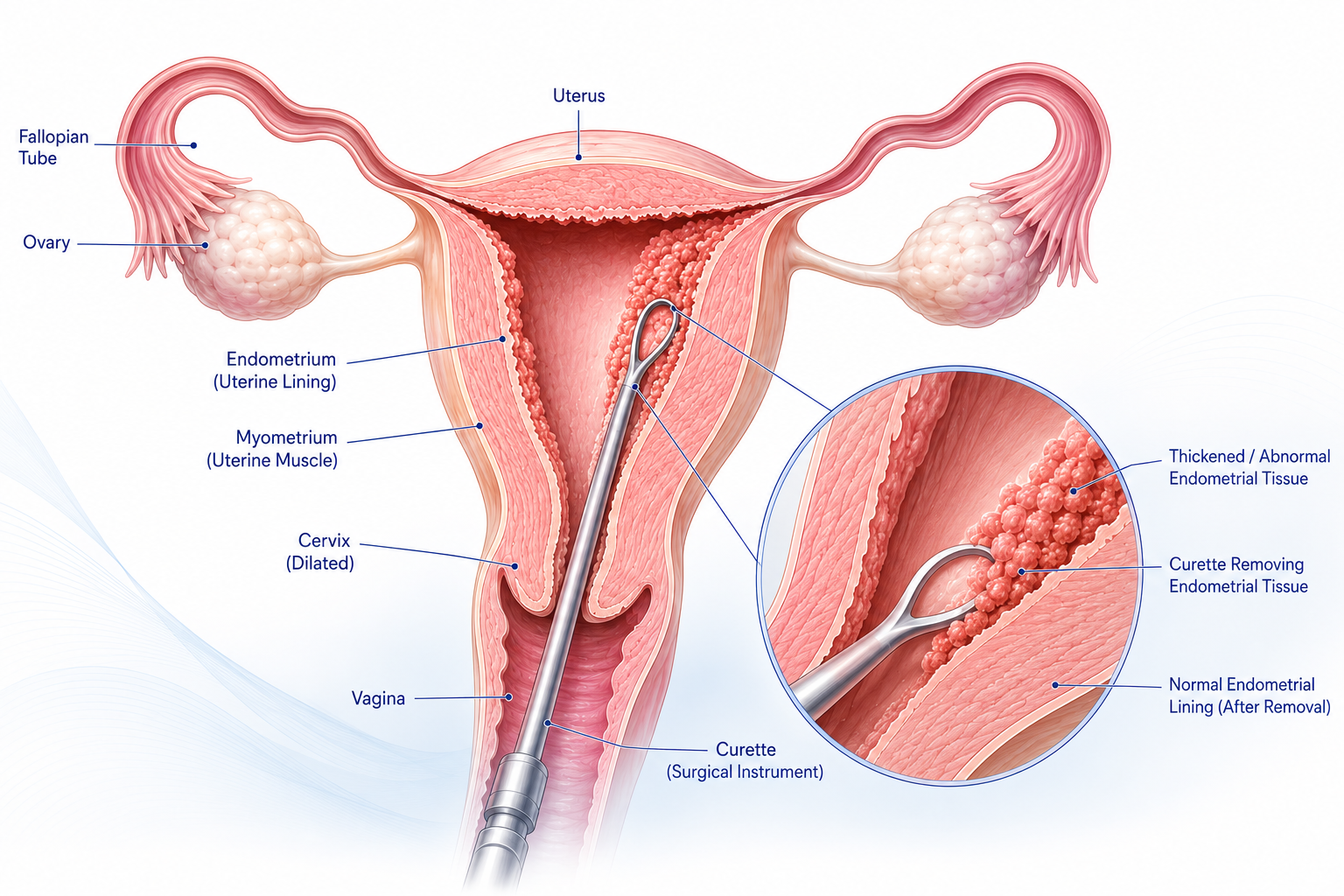
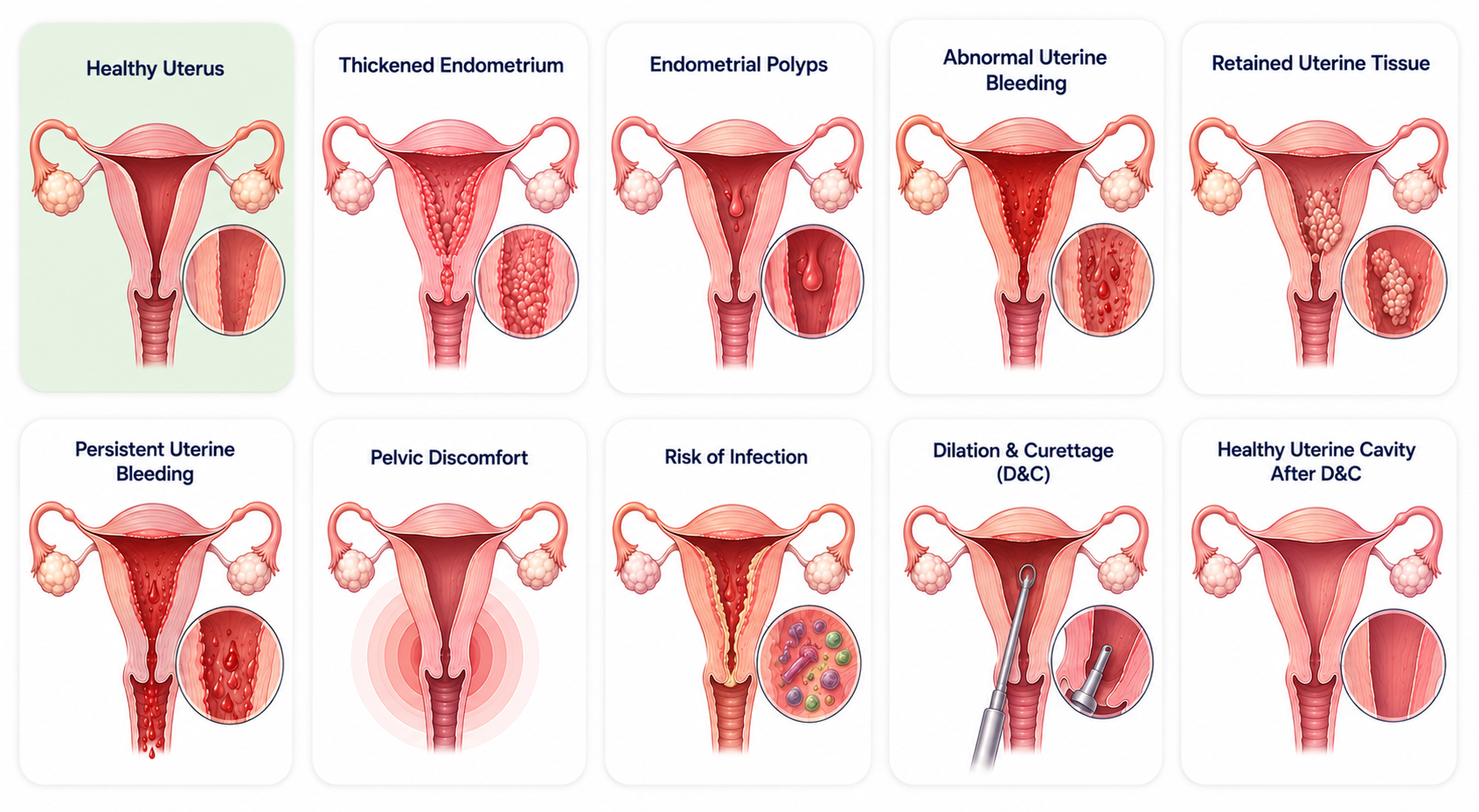
What Is Happening Inside Your Body?
The uterus is lined by a specialized, vascular tissue layer called the endometrium. This lining expands and builds up each month under hormone control, shedding naturally during normal menstruation if a pregnancy does not occur.
Sometimes the uterine lining undergoes abnormal metabolic changes, causing it to become thick, grow vascular polyps, bleed out of cycle, or fail to clear away after a miscarriage or childbirth event.
When baseline structural clearing mechanisms fail, patients experience ongoing symptoms such as intense bleeding, irregular cycle intervals, painful deep pelvic discomfort, prolonged trailing bleeding, or the presence of persistent pregnancy tissue fragments locked within the uterus canal.
If unviable tissue layers remain stuck inside the uterus for too long, they present risk paths for chronic hemorrhage, intrauterine bacterial infection, deep cramping pain, or create barriers for doctors trying to diagnose an underlying pre-cancer development.
An operative D&C solves this by physically evacuating the retained or hyperplastic tissue sheets, enabling the uterus to heal cleanly, ending the bleeding trajectory, and providing definitive tissue segments for pathology cell checks.
What Is Dilation & Curettage (D&C)?
Dilation and Curettage (D&C) is a brief, minor gynaecological procedure where the cervix is carefully dilated to insert narrow medical instruments, allowing the surgeon to clear abnormal tissue layers from the lining of the uterus.
Clinicians implement this procedure across standard scenarios to accurately diagnose unexplained bleeding sources, remove stubborn retained pregnancy structures, manage incomplete losses, scrape away hyperplastic lining paths, or secure high-quality tissue segments for pathology testing.
Once completed, the harvested cell layers are sent straight to a pathology laboratory for deep diagnostic review under a microscope.
The typical expected clinical outcomes include definitive control over dysfunctional bleeding, safe removal of stuck tissue, complete relief from structural pelvic symptoms, accurate staging of uterine conditions, and the mitigation of secondary infection vectors.
Benefits of the Procedure
- Stops abnormal uterine bleeding patterns safely
- Clears out unviable retained pregnancy tissue segments
- Prevents secondary bacterial intrauterine infections
- Helps diagnose complex uterine tissue abnormalities
- Provides clean tissue samples for pathology analysis
- Improves overall pelvic comfort and patient quality of life
- Reduces complication paths related to hidden retained structures
- Facilitates physiological healing after a miscarriage
- Supports clean reproductive recovery planning
.png)
Do You Really Need Surgery?
A gynecologist will recommend a D&C procedure when uterine bleeding profiles cannot be defined by standard clinical steps, pelvic scans show an overdeveloped endometrium, a miscarriage remains incomplete with dangerous retained tissue clusters, postmenopausal bleeding needs tracking, or suspected cellular mutations require complete pathology verification.
Alternative Treatments
Depending on the condition, alternatives may include:
Medications
- Hormonal line therapies to balance cycle flows
- Targeted progesterone treatments to control hyperplastic growth
- Birth control pill configurations to stabilize ovulation bleeding
- Antifibrinolytic medicines to reduce acute volume loss
Observation (Expectant Management)
This pathway is suitable primarily when the abnormal bleeding is exceptionally mild, ultrasound confirms that early miscarriage tissue may pass safely and naturally without intervention, or clinical symptoms show active improvement day-over-day.
Hysteroscopy Extraction Alternatives
This direct endoscopic alternative allows complete visual exploration of the intrauterine architecture, enabling the targeted excision of isolated structural changes like localized polyps or small fibroids without requiring random scraping.
Lifestyle Measures Limitations
While regular diet shifts and tracking help baseline metabolic health, they completely lack the capacity to clear adherent pregnancy tissue, remove fibrous polyps, or solve diagnostic questions regarding mutated lining cells.
Please note that alternative conservative pathways are completely contraindicated when patients present with severe uterine hemorrhaging, clinical pelvic infection, large volume retained structures, or strong high-risk markers for reproductive cancers.
When Should You Consult a Specialist?
Schedule a specialized evaluation with a gynecologist immediately if you experience heavy prolonged menstrual flows, fresh or dark vaginal bleeding long after completing menopause, repeated miscarriage patterns, persistent tracking bleeding following a pregnancy loss event, abnormal dense ultrasound findings, severe localized pelvic pain alongside spotting, ongoing fertility difficulties, or if you suspect hidden retained structures after a delivery.
When Should You Not Delay Treatment?
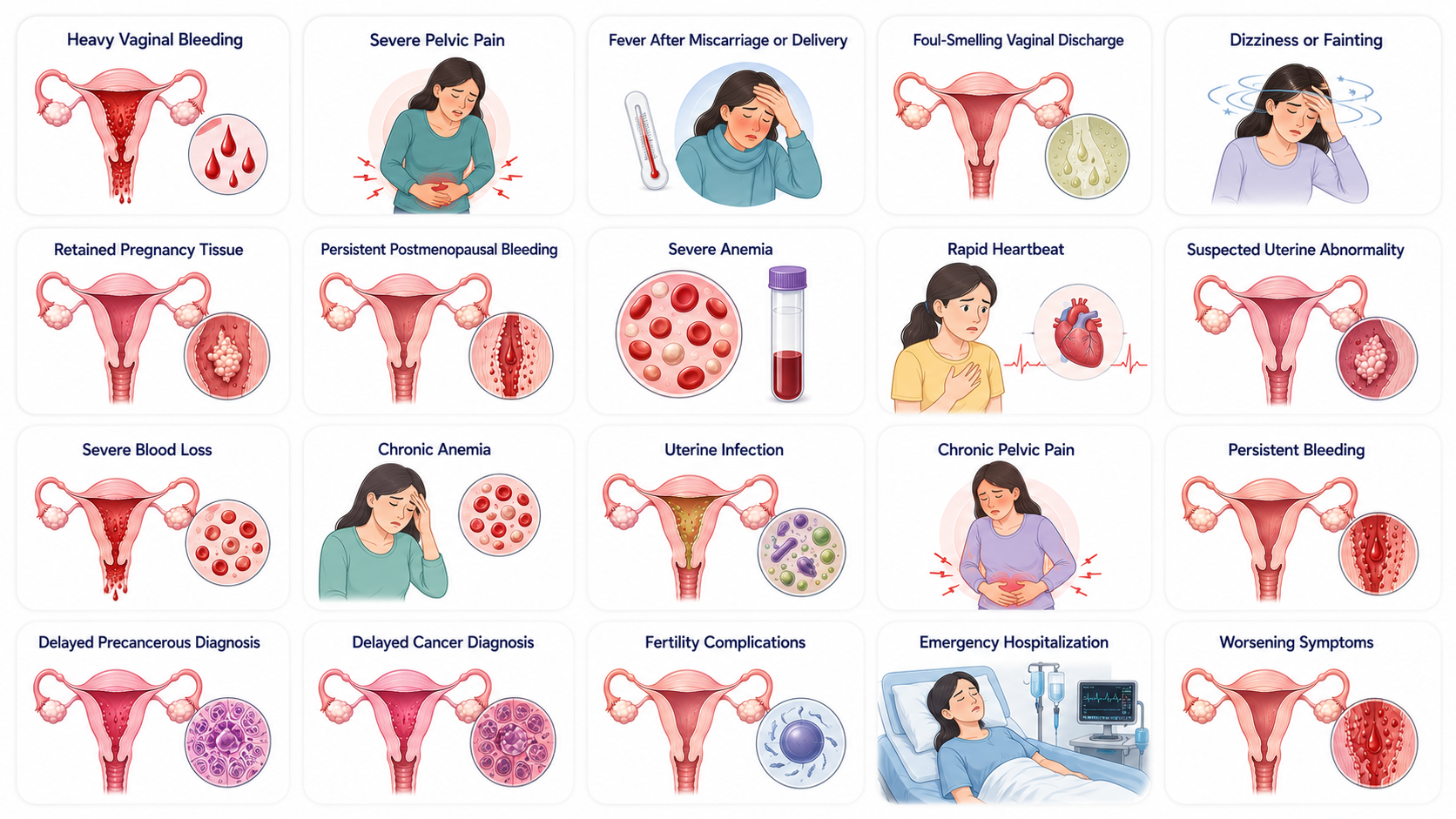
Seek emergency medical evaluation immediately if you develop any of these high-risk acute clinical markers:
- Heavy bleeding that completely soaks through multiple standard pads per hour
- Severe, unmanageable lower abdominal or deep pelvic pain
- High fever, chills, or shaking attacks following a recent miscarriage or delivery
- Foul-smelling, green, or yellow purulent vaginal discharge
- Sudden waves of dizziness, cold sweats, confusion, or fainting spells
- Known or suspected retained pregnancy tissue causing systemic changes
- Fresh, bright-red persistent bleeding occurring after menopause
- Severe anemia signs like blue-tinted lips, breathing gasps, or extreme weakness
- A rapid, racing heartbeat paired with an ongoing heavy bleed profile
- Acute hemorrhage associated with ultrasound-verified complex uterine masses
Risks of Delaying Treatment
Postponing a recommended surgical clearance carries serious clinical risk trajectories, including life-threatening blood volume loss, acute or chronic iron-deficiency anemia, systemic uterine or fallopian tube infections (sepsis), chronic irreversible pelvic pain syndromes, persistent exhausting bleeding phases, delayed staging of precancerous endometrial hyperplasia changes, delayed diagnosis of treatable reproductive cancers, permanent internal scarring or fertility complications, repeatable emergency room hospital admissions, and progressive worsening of basic pelvic conditions.
Know Your Insurance Benefits
Get clarity on your insurance coverage before your treatment, with guidance from our care team every step of the way.
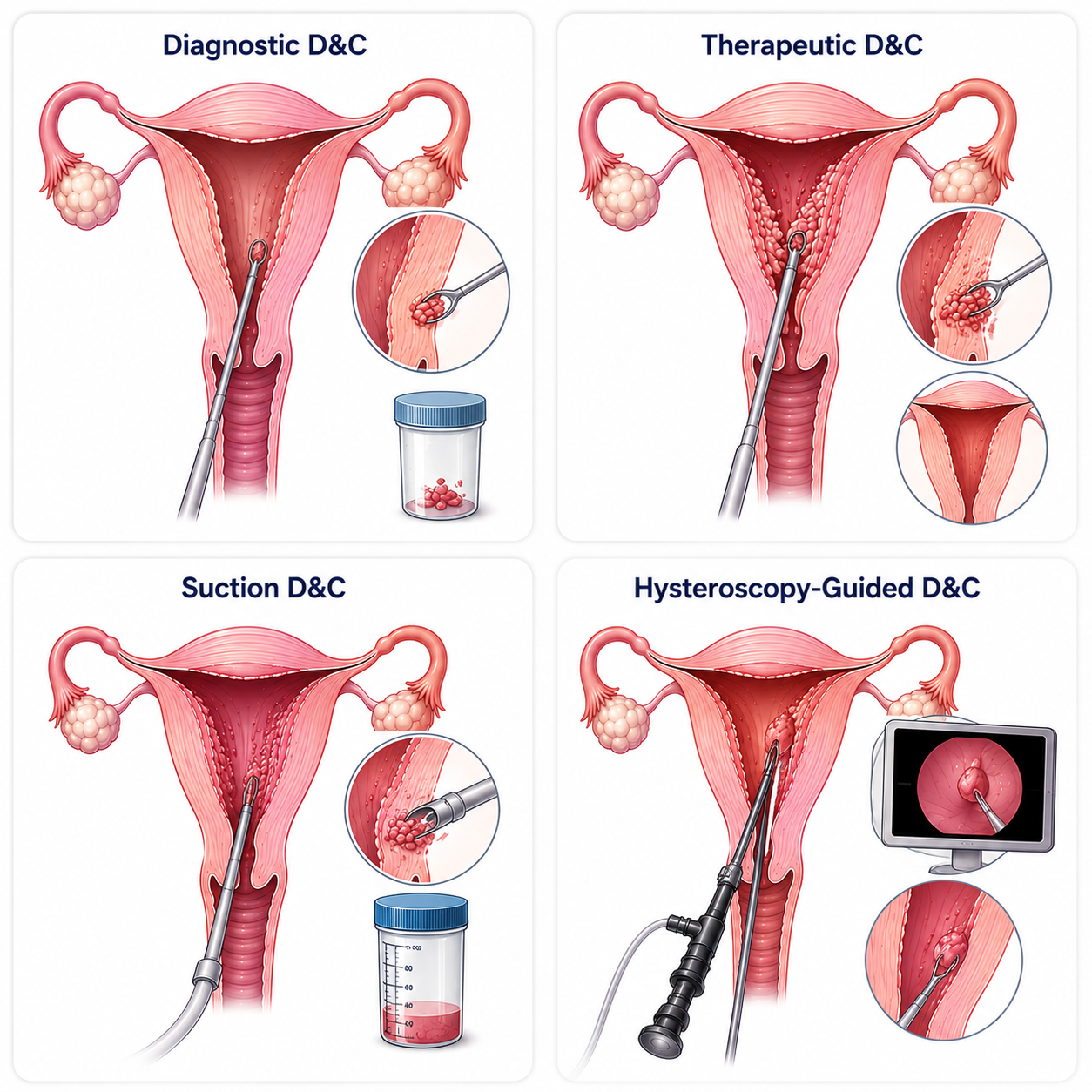
Check My Insurance BenefitsTypes of Procedures Available
Diagnostic D&C
This procedure focuses on collecting precise tissue samples from the lining to investigate abnormal cycles or postmenopausal bleeding.
- Benefits, helps identify hidden causes of abnormal bleeding, catches hyperplastic cell mutations early, and guides future medication protocols
- Limitations, primarily functions as an investigative step and does not cure systemic hormonal disorders
- Best For, patients with unexplained abnormal uterine bleeding profiles requiring cell classification
Therapeutic D&C
Performed explicitly to empty the uterine cavity and clear out structures driving acute clinical symptoms.
- Benefits, instantly stops active hemorrhaging, clears complex retained tissues cleanly, and provides fast symptom relief
- Limitations, does not prevent future recurrence of structural anomalies like new polyp formation
- Best For, patients presenting with stuck post-pregnancy tissue or extreme acute blood loss stages
Suction D&C (Aspiration)
Implements a gentle vacuum suction mechanism to cleanly clear out the uterine contents.
- Benefits, presents significantly less mechanical trauma risks to the uterine wall layer and enables rapid physical recovery
- Limitations, unsuitable for scraping dense, heavily calcified structural path masses
- Best For, patients requiring complete evacuation of soft retained pregnancy tissue after early loss
Hysteroscopy-Guided D&C
Combines traditional curettage with an endoscope console camera for real-time interior tracking.
- Benefits, exceptional precision through direct visual tracking, ensuring zero blind scraping spots and safer tissue margins
- Limitations, requires specialized surgical tower tech and carries slightly higher baseline procedure costs
- Best For, patients with tiny localized polyps, complex recurrent histories, or anomalous lining changes
Comparison of Different Treatment Options
Doctor's Recommendation
Doctors often recommend a D&C when surgical tissue removal is necessary, when bleeding is heavy, or when a tissue sample is required for diagnosis. The best treatment choice depends on the patient's age, clinical symptoms, future fertility plans, and the underlying condition.
Preparing for Surgery
Before scheduling your procedure, standard pre-operative clearing investigations include a complete blood count (CBC) to cross-check blood health, cross-matching blood grouping parameters, baseline blood sugar testing, a confirmatory pregnancy test, a pelvic ultrasound scan to localize anomalies, and a full coagulation profile to ensure clotting channels function safely.
Inform your doctor about all daily medications, including prescription blood thinners that must be paused, diabetes medications requiring pre-op scheduling, heart medications needing tracking adjustments, as well as any over-the-counter herbal supplements or known medication allergy history.
To prepare smoothly, follow your precise pre-anesthesia fasting instructions (nothing by mouth for 6–8 hours), stop smoking as early as possible before your slot, avoid alcohol intake, arrange a trusted family member for transportation home, and wear loose, comfortable clothing to the hospital facility.
What Happens on Surgery Day?
- Completing hospital registration and pre-op check-in formalities
- Nursing review of medical history records and current vitals
- Signing the informed surgical consent documents
- Initiating a standard IV line for procedural hydration and medications
- Final pre-operative anesthesia evaluation in the holding area
- Targeted sedation or general anesthesia is safely administered through your IV line.
- The surgeon cleans the vaginal canal and gently expands the cervical opening using smooth dilator rods.
- Specialized instruments or thin suction aspiration catheters are introduced through the open cervix.
- The target tissue layer is carefully removed from the inner uterine wall bed.
- The harvested tissue samples are preserved and labeled for laboratory analysis.
- The surgical area is checked to verify complete tissue clearance and safe clotting.
- Instruments are removed smoothly, signaling the formal completion of the procedure.
- Resting comfortably under close monitoring in the recovery room block
- Frequent checks of blood pressure, pulse, and oxygen saturation parameters
- Evaluating post-op pain levels and administering initial oral medications
- Receiving safe same-day discharge clearance once you can walk and pass urine
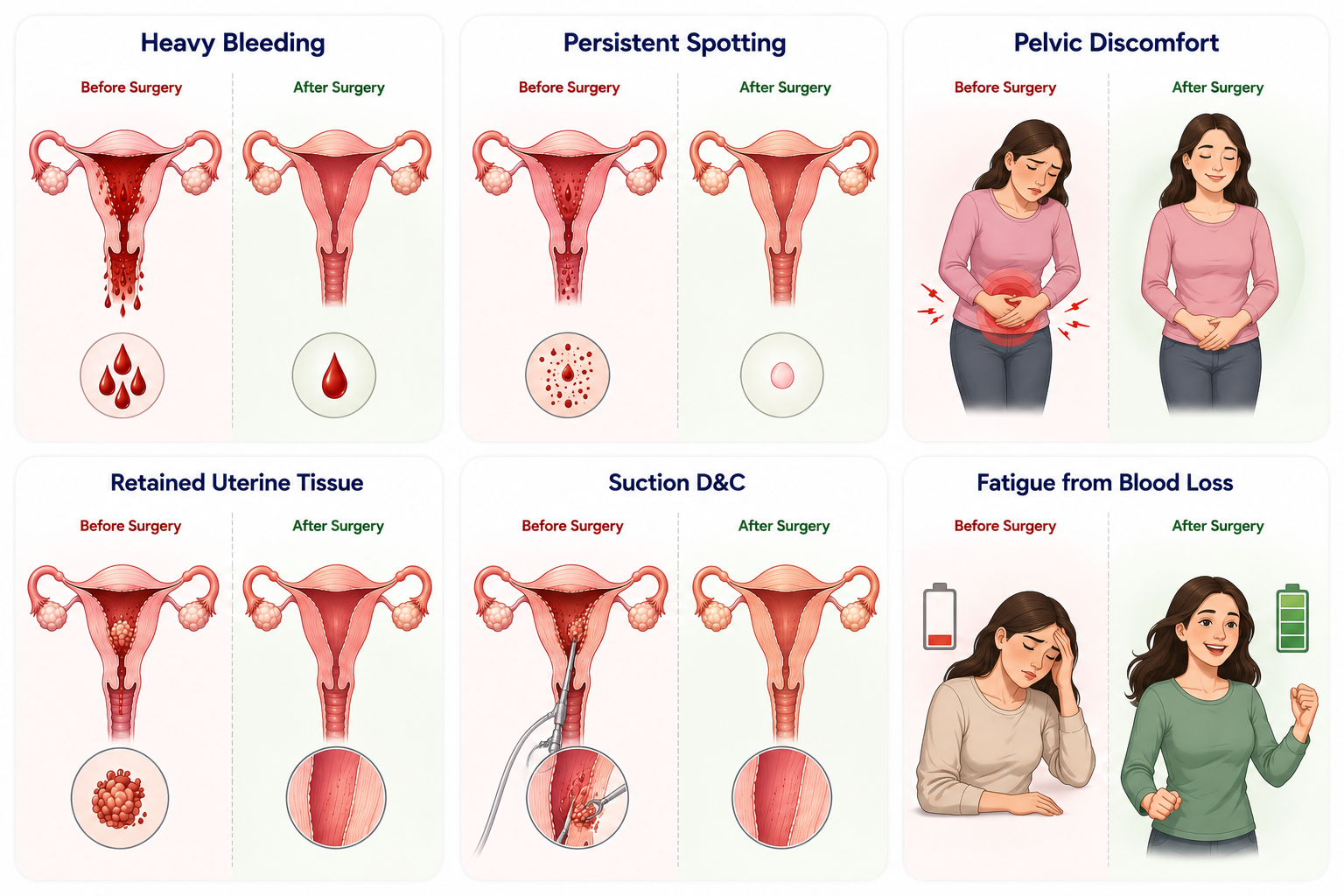
Before vs After Surgery
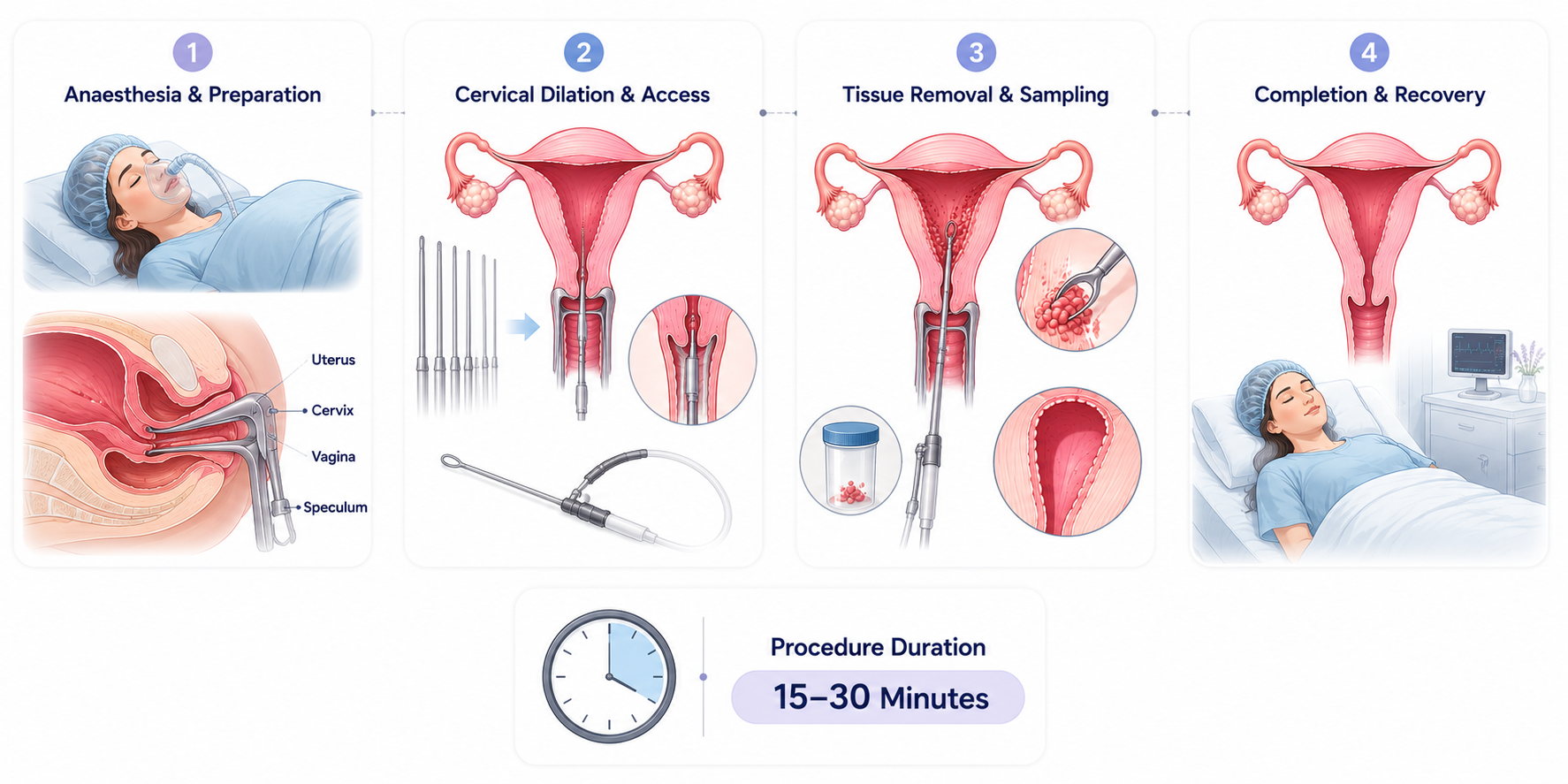
How Is the Surgery Performed?
Step 1
Step 1
Anaesthesia and Preparation
The patient receives anesthesia and a speculum is inserted into the vagina.
Patient receives anesthesia.
A speculum is inserted into the vagina.
Step 2
Step 2
Cervical Dilation and Access
The cervix is gradually dilated and a curette or suction device is introduced.
The cervix is gradually dilated.
Curette or suction device is introduced.
Step 3
Step 3
Tissue Removal and Sampling
The uterine lining or retained tissue is removed, the cavity is checked, and tissue is collected for testing if needed.
Uterine lining or retained tissue is removed.
The cavity is checked for completeness.
Tissue is collected for testing if needed.
Step 4
Step 4
Completion and Recovery
The instruments are removed and the patient is moved to recovery.
Instruments are removed.
Patient is moved to recovery.
Duration: Most D&C procedures take approximately 15–30 minutes.
Expert Guidance, Every Step of the Way
Our dedicated care coordinators are here to answer your questions and guide you through every stage of your treatment.
Talk to Our ExpertsPossible Risks and Complications
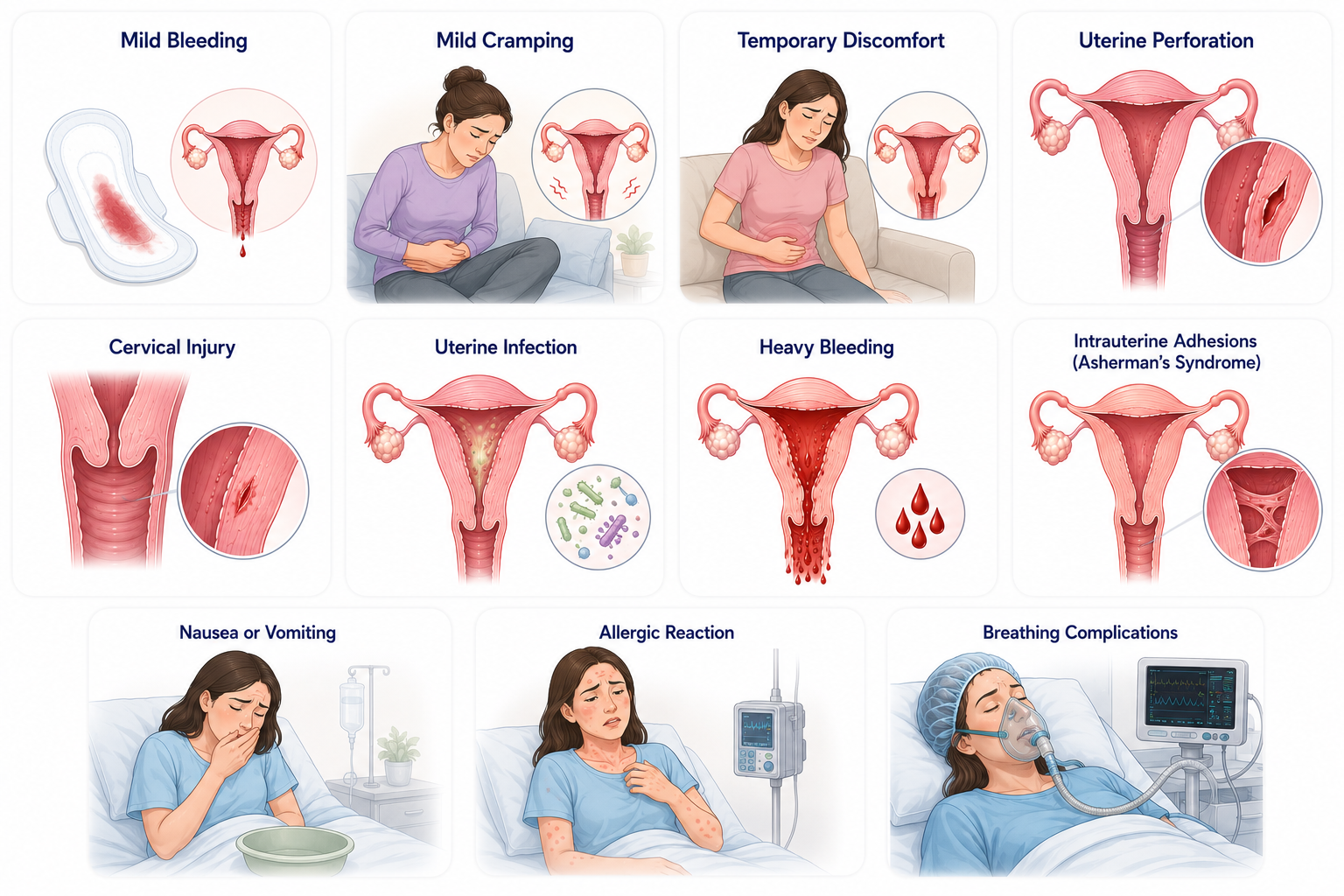
Like all operative diagnostic procedures, a D&C carries specific risk tracks. While serious problems remain highly uncommon, understanding potential events helps ensure safe post-op tracking:
1. Common Operational Effects
- Mild cramping, temporary baseline uterine contracting as the muscle layer adjusts post-clearance
- Light spotting, expected minor blood trailing or discharge lasting for a few days up to two weeks
- Temporary discomfort, mild localized pressure across the lower pelvis that responds well to oral tablets
2. Rare Surgical Complications
- Uterine perforation, an accidental small puncture in the uterine wall by an instrument, usually resolving with monitoring
- Cervical injury, minor tearing or trauma to the cervix tissue during the mechanical dilation phase
- Endometrial infection, secondary intrauterine infection introducing lower stomach soreness and fever risks
- Excessive hemorrhage, unexpected heavy bleeding during or after scraping, occasionally needing intervention
- Asherman's syndrome, rare development of intrauterine scar tissue adhesions following aggressive sharp curettage
3. Anesthesia Specific Risks
- Post-op nausea, temporary stomach tracking upset or vomiting as sedation compounds leave the blood
- Allergic reactions, unexpected hypersensitivity responses to systemic drugs, managed instantly by care teams
- Respiratory depression, very rare breathing rate slows during deep sedation pathways needing temporary supportive oxygen
Statistical Risk Frequency Overview
Recovery Timeline & Clinical Expectations
Postoperative Care Protocols
Monitoring parameters: Immediate post-procedure care focuses on tracking vital signs, running pad checks to assess bleeding, and scoring baseline pain levels dynamically.
Pain management: Administering fast-acting oral pain medications and anti-inflammatory compounds before setting up your discharge package.
Mobility tracks: Encouraging light bedside walking sessions as soon as anesthesia sedation wears off completely.
Hygiene management: Since no external wounds exist, focus completely on tracking discharge volume and avoiding tampons or internal douches entirely.
Nutritional support: Prioritize high-fluid intake alongside iron-rich meals to rebuild red cells if substantial blood loss occurred prior to your procedure.
Personal recovery rules: Always implement sanitary pads instead of tampons, maintain strict genital cleanliness, and follow specific doctor guidance regarding home bathing.
Permitted movements: Gentle short walks inside the home and basic desk tasks are fully safe within 24–48 hours.
Prohibited actions: Strictly avoid sexual intercourse, tampon insertion, swimming pool exposure, heavy weight lifting, or strenuous core exercise until cleared by your gynaecologist.
Follow-Up Scheduled Reviews
Your standard postoperative recovery schedule incorporates a vital clinic review within 1–2 weeks to check internal contraction patterns, explore the detailed path lab tissue report, address any lingering spotting signs, and build further medication or fertility tracking options if required.
Warning Signs After Surgery
Seek immediate professional medical attention at our facility if you develop any of these tracking warning flags:
- A sudden fever spike climbing above 100.4°F (38°C).
- Acute, worsening lower abdominal pain or pelvic spasms.
- Heavy bright-red vaginal bleeding requiring multiple pad changes per hour.
- Passing unusually large or painful blood clots.
- Foul-smelling, persistent, or unusual vaginal discharge.
- Severe waves of dizziness, cold syncopes, or fainting spells.
- Acute chest pressure or sudden difficulty breathing.
- Unresolved nausea or persistent vomiting cycles lasting over 24 hours.
- Progressive, painful lower abdominal swelling or distension.
- Inability to pass urine comfortably within 12 hours of returning home.

Recent Clinical Studies Redefining Dilation & Curettage (D&C)
Recent evidence has refined the role of Dilation & Curettage (D&C) in modern gynecology. Current international guidelines recommend individualized management for miscarriage, abnormal uterine bleeding, and endometrial evaluation, with D&C reserved for carefully selected patients when medical or expectant management is unsuitable or when diagnostic tissue sampling is required. Contemporary practice also emphasizes ultrasound guidance, patient-centered counseling, and minimally invasive alternatives whenever appropriate.
Questions to Ask Your Surgeon
- Why am I being advised to undergo a D&C?
- What condition are you trying to diagnose or treat?
- Are there alternatives to surgery?
- What type of anesthesia will be used?
- What are the risks in my case?
- Will tissue be sent for testing?
- How long will recovery take?
- When can I return to work?
- Will this affect future fertility?
- When can I exercise again?
- How much bleeding is normal afterward?
- What warning signs should I watch for?
Frequently Asked Questions
Is D&C painful?
The procedure is usually performed under anesthesia, so you should not feel pain during surgery.
How long does a D&C take?
Typically 15–30 minutes.
Is hospital admission required?
Most patients go home the same day.
How long will bleeding last?
Light bleeding may continue for several days to two weeks.
When can I return to work?
Many patients return within 1–3 days depending on recovery.
Will D&C affect fertility?
Most women maintain normal fertility after a D&C.
Can I become pregnant again after D&C?
Yes, many women successfully conceive afterward.
When can I have sexual intercourse?
Usually after bleeding stops and your doctor approves.
Is D&C safe?
It is generally considered a safe and commonly performed procedure.
Why is tissue sent for testing?
To identify abnormal cells, polyps, hyperplasia, or other conditions.
What anesthesia is used?
General anesthesia, sedation, or regional anesthesia may be used.
How successful is D&C?
Success rates are generally above 95% when appropriately indicated.
Can bleeding return after D&C?
It depends on the underlying condition. Some conditions may recur.
Does insurance cover hysterectomy?
Most medically necessary procedures are covered.
Can I travel after surgery?
Short travel is usually possible within a few days if recovery is smooth.
Can I exercise after D&C?
Light walking is encouraged, but strenuous exercise should wait until cleared.
What foods should I eat after surgery?
A balanced diet rich in fluids, iron, protein, fruits, and vegetables.
What are the signs of infection?
Fever, worsening pain, foul-smelling discharge, and increasing bleeding.
Will I need another D&C?
Most patients do not, but it depends on the underlying condition.
When will my next period occur?
Usually within 4–8 weeks, although timing varies.
Find the Right Specialist
A D&C is typically performed by a gynecologist or obstetrician-gynecologist. SPEROW aligns your care pathway with elite, high-volume specialists attached to dedicated surgical facilities offering full daycare amenities and simplified health insurance claim authorizations.

N V Gowthami Mullangi
VerifiedGynecology
Experience: 15+ Yrs
Hospital: Cygnet Clinics
Languages: Eng
Advanced Surgical Care
Book ConsultationView Profile 
P Farida
VerifiedGynecology
Experience: 10+ Yrs
Hospital: Renova Neelima
Languages: Eng
Advanced Surgical Care
Book ConsultationView Profile 
Reeta Agarwal
VerifiedGynecology
Experience: 23+ Yrs
Hospital: Renova Neelima
Languages: Eng
Advanced Surgical Care
Book ConsultationView Profile
Find a Surgeon You Can Trust
We'll connect you with an experienced specialist who matches your condition, treatment needs, and preferences.
Find the Right SurgeonFree Consultation
FreeGet connected with a trusted doctor for an expert second opinion through our care team.
No Cost Expert Guidance · Coordinated Care · Personalized Support