Hysteroscopy
A complete, patient-centered guide to hysteroscopy — indications, procedure types, recovery milestones, risks, insurance coverage, and costs in India.
Hysteroscopy
A complete, patient-centered guide to hysteroscopy — indications, procedure types, recovery milestones, risks, insurance coverage, and costs in India.
Medically Reviewed ByDr. N V Gowthami MullangiLast updated: 16 July 2026Free Second Opinion
Get connected with a trusted doctor for an expert second opinion through our care team—at no cost.
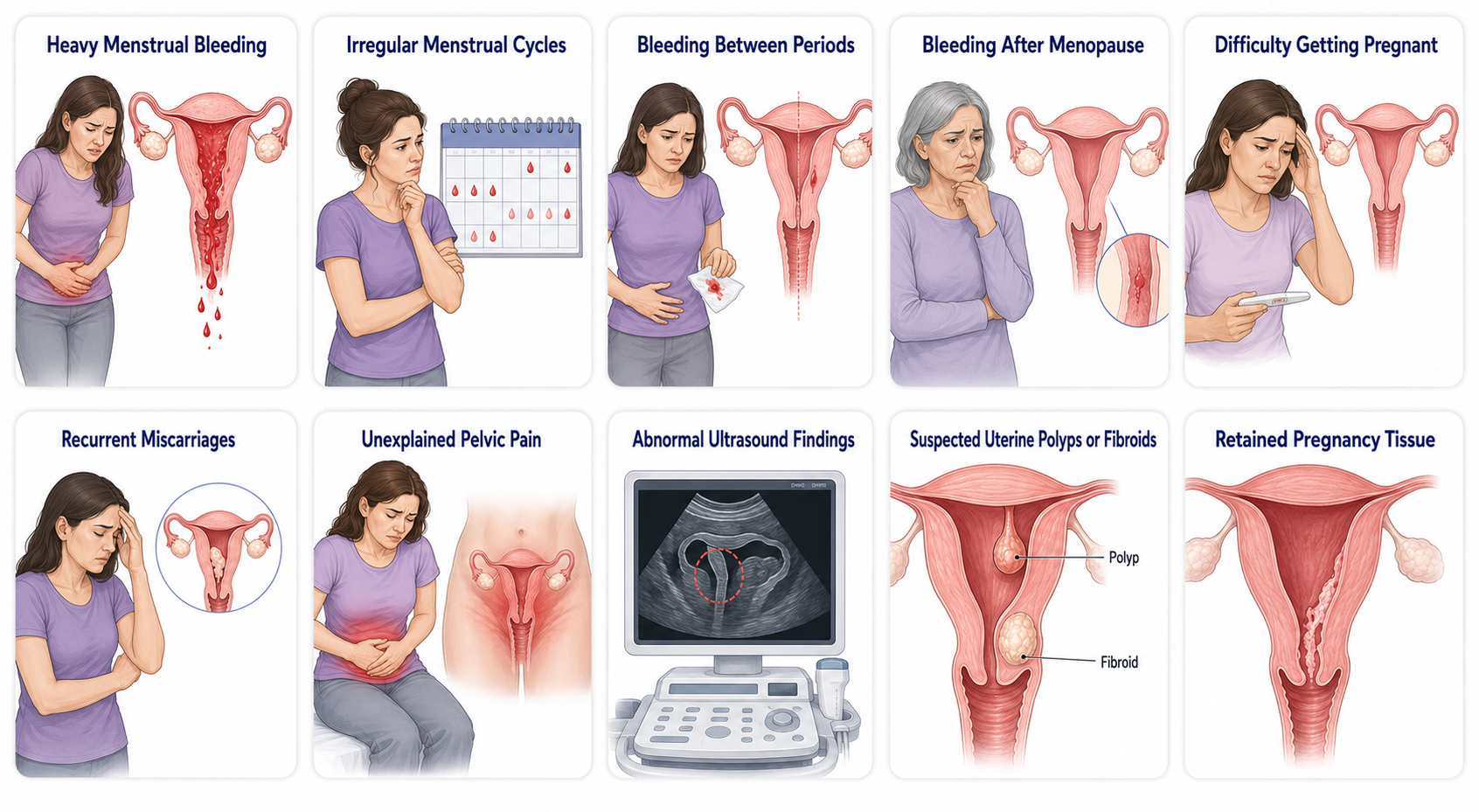
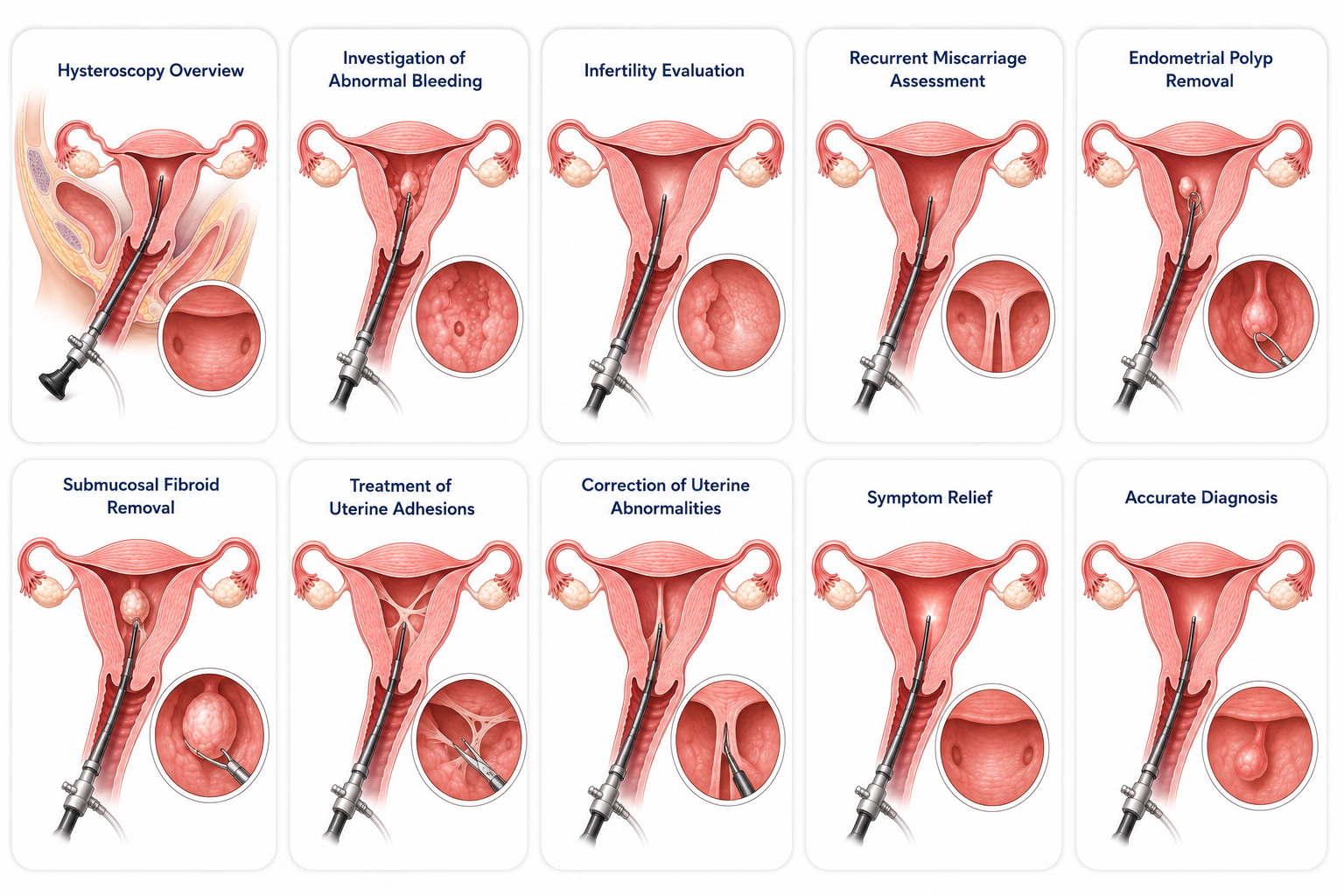
Clinical Indications for a Hysteroscopy
A hysteroscopy is typically advised when a patient presents with unresolved pelvic symptoms or reproductive challenges that require high-precision internal assessment:
1. Dysfunctional Bleeding Signifiers
- Menorrhagia, abnormally heavy or prolonged menstrual bleeding that disrupts regular routines
- Oligomenorrhea, highly irregular menstrual cycles with unpredictable flow variations
- Intermenstrual tracking, unexpected bleeding or spotting occurring actively between defined periods
- Postmenopausal bleeding, any form of fresh vaginal bleeding occurring long after menopause, requiring prompt investigation
2. Reproductive & Structural Indicators
- Primary/Secondary infertility, difficulty getting pregnant despite regular unassisted attempts
- Recurrent loss, recurrent miscarriages that necessitate a structural look at the cavity lining
- Intractable pain, unexplained pelvic pain or cramping unrelated to clear external anomalies
3. Radiographic Discrepancies
- Intrauterine filling defects, abnormal ultrasound or scan findings localized inside the uterine lining walls
- Suspected growths, strong diagnostic suspicion of hidden endometrial polyps or submucosal fibroids
- Retained tissue profiles, retained products of conception remaining behind after a miscarriage or delivery event
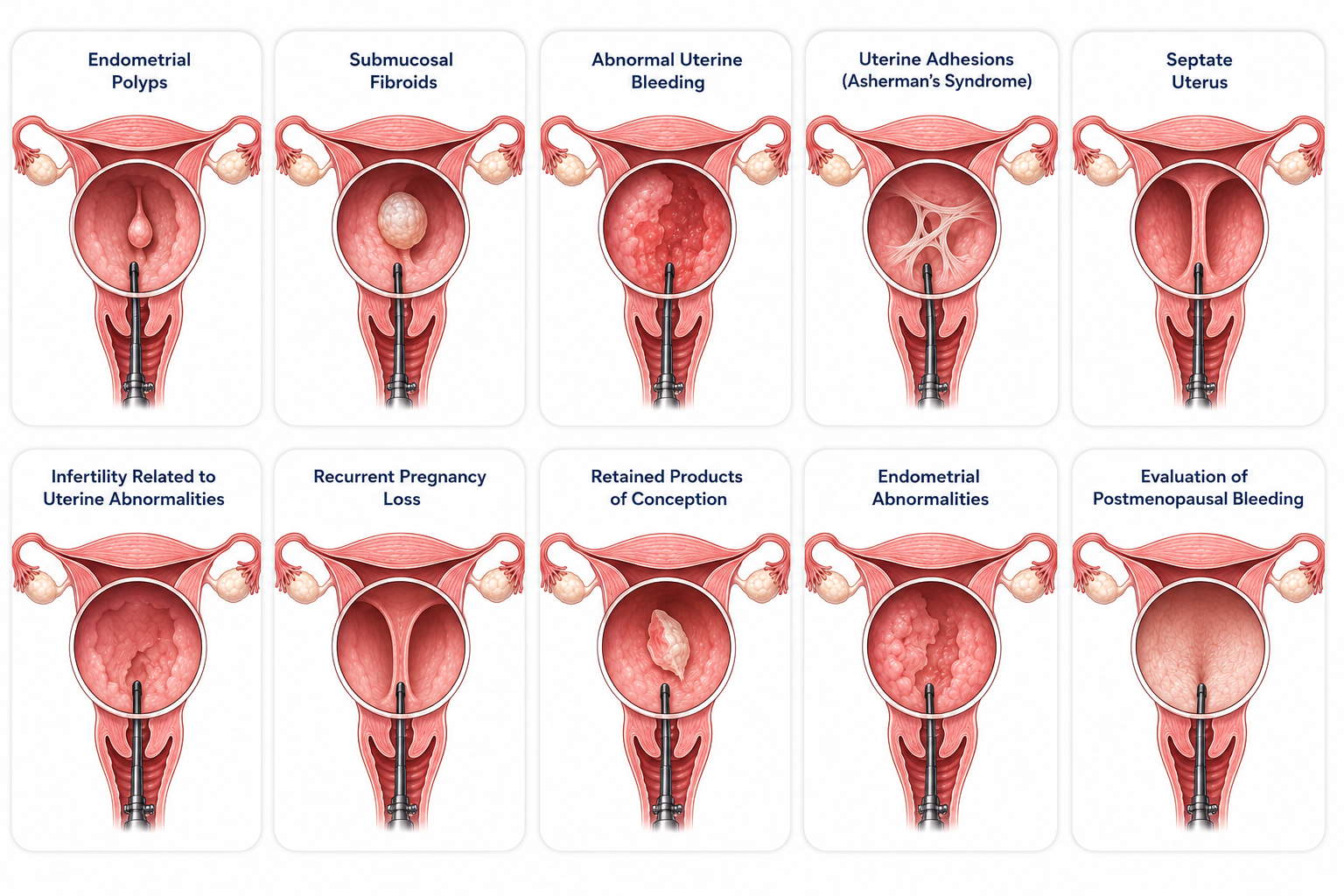
Common Conditions Treated
1. Benign Intrauterine Growths
- Endometrial polyps, soft vascular growths on the inner lining that trigger heavy bleeding and spot anomalies
- Submucosal fibroids, benign muscular tumors that project directly into the cavity, distorting its shape
- Abnormal uterine bleeding, AUB conditions driven by localized cellular changes inside the endometrium lining layers
2. Structural & Reproductive Pathologies
- Asherman's syndrome, dense uterine adhesions or scar tissue bands that bond cavity walls together
- Septate uterus, a congenital tissue wedge splitting the uterus down the center, heavily associated with recurrent early pregnancy losses
- Uterine infertility factors, localized architectural abnormalities blocking normal gamete migration or embryonic nesting
- Retained tissue products, products of conception remaining attached to the internal muscle wall after pregnancy resolution
- Endometrial hyperplasia staging, abnormal thickening of the uterine lining demanding directed visualization and testing checks
- Postmenopausal anomalies, comprehensive endo-cavity mapping to verify unexpected postmenopausal bleeding sources
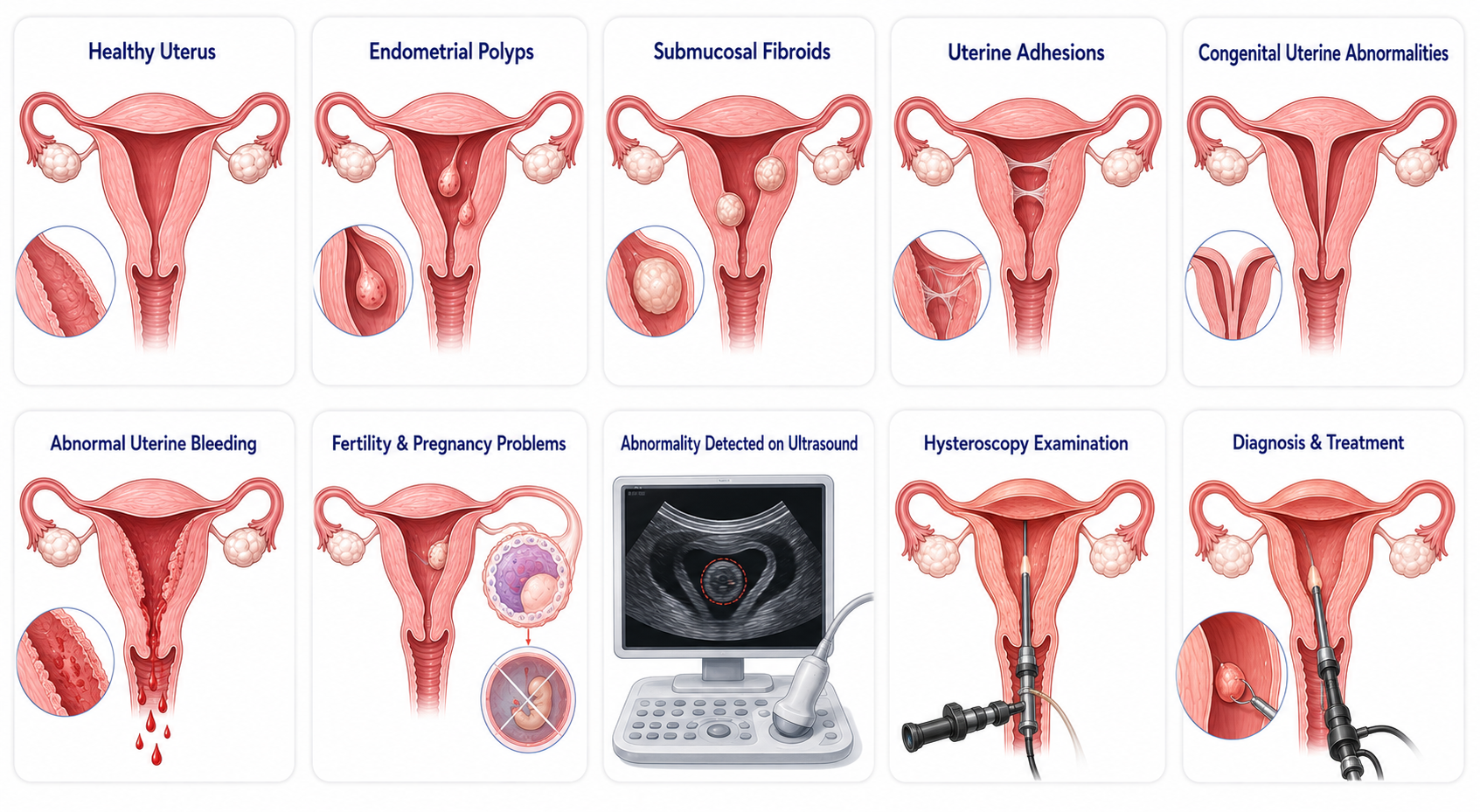
What Is Happening Inside Your Body?
The uterus is a muscular reproductive organ lined internally by a dedicated responsive tissue layer called the endometrium. This lining layer naturally expands, transitions, and sloughs off each month during standard menstruation cycles.
Sometimes, abnormal localized growths, fibrous scar tissue planes, congenital septums, or stubborn unviable tissue strings collect inside the cavity, preventing the organ from contracting effectively or disrupting the smooth tracking of embryo implantation.
Standard ultrasound scans help pick up general signs of these abnormalities, but blind procedures risk missing small pathologies or leaving behind marginal edges. A hysteroscopy solves this bottleneck by providing a highly clear, high-definition direct view, allowing doctors to diagnose anomalies confidently and address them with targeted precision during the same session.
What Causes These Endometrial Anomalies?
The internal structural anomalies that necessitate a diagnostic or operative hysteroscopy are typically triggered by specific underlying paths:
- Hormonal surges, unregulated estrogen levels stimulate focal tissue sites to expand rapidly, forming polyps or leiomyomas
- Post-procedural scarring, prior blind curettage or clinical infections can scar the sensitive muscle walls, developing dense fibrous bands
- Congenital variations, embryonic development variations can leave an avascular muscular septum partitioning the central cavity space
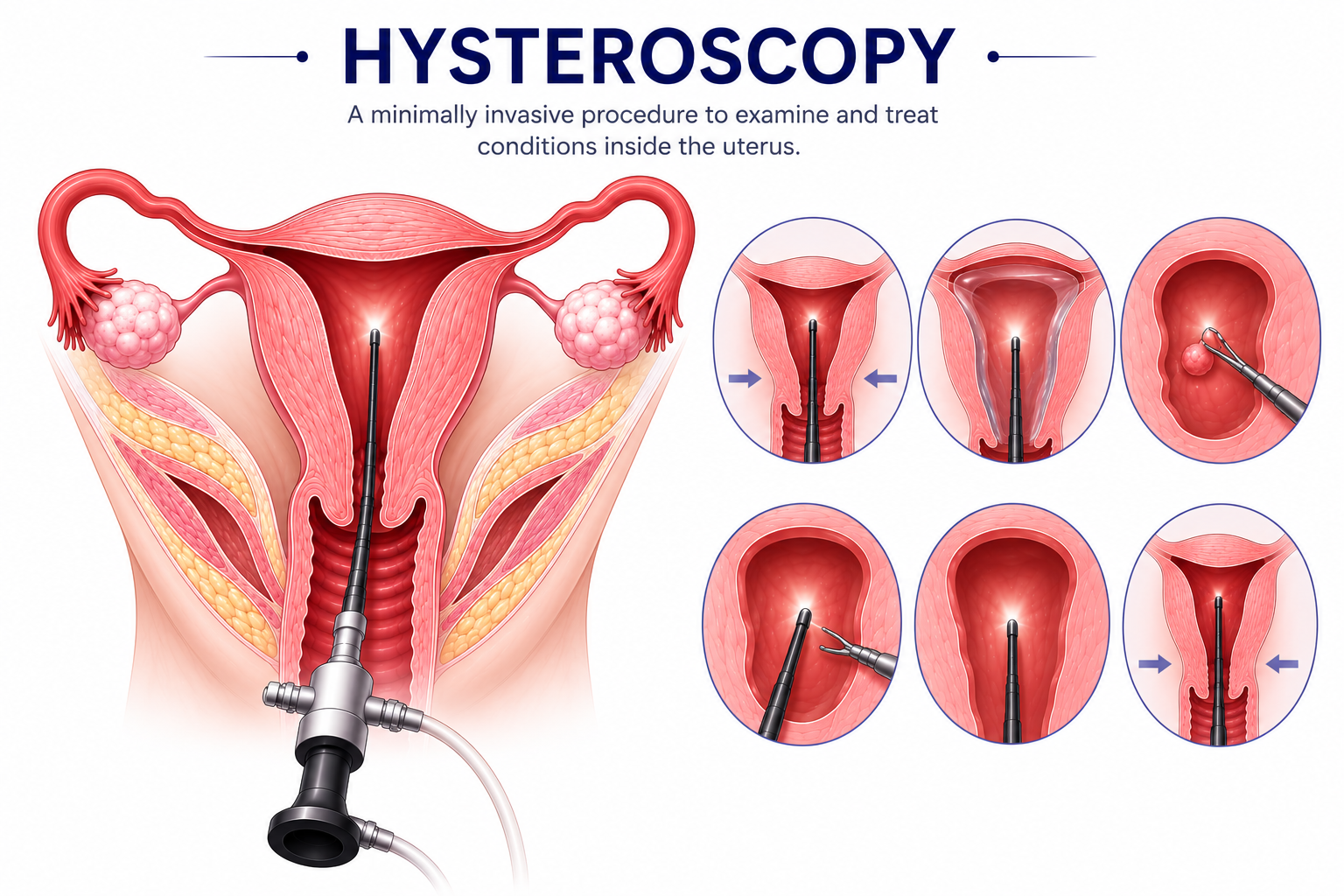
What Is Hysteroscopy?
Hysteroscopy is an advanced, minimally invasive gynaecological intervention executed to carefully view the internal architecture of the uterine cavity.
By inserting an ultra-thin, lighted camera console called a hysteroscope gently through the natural vaginal track and cervix, surgeons gain comprehensive visual mastery of the internal environment. Because this approach leverages natural openings, it eliminates the need for any external skin cuts or sutures.
The procedure maps out excellent recovery benchmarks across five core operational priorities: rapidly confirming obscure abnormal bleeding sources, mapping out hidden blocks during comprehensive infertility screening, clearing structural lining barriers like hyperplastic polyps or submucosal fibroid nodes, severing restrictive scar tissue matrices safely, and correcting deep congenital septum errors.
Benefits of Hysteroscopy Surgery
- Complete absence of external abdominal cuts or surgical scarring
- Highly localized, minimally invasive procedure model
- Rapid postoperative recovery and brief down-time track
- Real-time, clear direct visualization of the deep uterine environment
- Exceptional diagnostic accuracy compared to blind testing tracks
- Simultaneous find-and-fix treatment capability in a single procedure
- Complete preservation of the uterus muscle layers for fertility goals
- Excellent long-term relief from heavy bleeding or tracking period pain
- Saves the patient from requiring far more invasive open surgeries later
- Brief daycare stay format with convenient same-day discharge
Do You Really Need Surgery?
A specialist will advise a hysteroscopy when pelvic imaging clearly identifies anomalous filling defects inside the cavity, heavy bleeding patterns resist medical management lines, advanced fertility screening requires direct lining evaluation, or recurrent early losses demand a complete architectural review.
Comparison of Different Treatment Options
Doctor's Recommendation
Gynaecologists favor hysteroscopy because its micro-visual access eliminates diagnostic guesswork. It allows the clinician to map the landscape clearly and treat structural issues during the same procedural timeline, maintaining structural safety for future pregnancy goals.
Types of Procedures Available
Hysteroscopic procedures are categorized based on whether the primary focus is investigative mapping, clinic-room intervention, or targeted operating room tissue removal:
- Diagnostic hysteroscopy, focused entirely on evaluating the cavity architecture using a thin diagnostic lens without removing tissue
- Operative hysteroscopy, utilizes specialized micro-shears or electrosurgical loops passing through the frame channel to correct structural pathologies
- Office hysteroscopy, a rapid, walk-in diagnostic review completed right in the clinic consultation room with minimal or no local numbing needed
- Hysteroscopic polypectomy, targeted excision where endometrial polyps are isolated and snipped cleanly away from their tissue base
- Hysteroscopic myomectomy, surgical shaving or removal of deep submucosal fibroids protruding into the open cavity interior
Preparing for Surgery
Standard tests required to verify baseline procedural safety include comprehensive blood panels, a pre-procedure pregnancy test, high-resolution ultrasound mapping, cardiorespiratory or ECG checks if indicated, and specialized uterine lining biopsies in select cases.
Be sure to notify your specialist regarding prescription blood thinners that require pausing, active diabetes medications needing scheduling adjustments, blood pressure drugs, or any over-the-counter herbal supplements.
Optimize your recovery path by cutting out smoking before your slot, avoiding alcohol intake, adhering strictly to your pre-anesthesia fasting window, and discussing future pregnancy timelines transparently with your specialist.
What Happens on Surgery Day?
- Completing the hospital registration and checking into your daycare block
- Detailed clinical review of your medical history file and active vitals tracking
- Verification and signing of the procedural consent paperwork
- Setting up a standard IV portal line for surgical medications and antibiotics
- Preoperative anesthesia review in the daycare holding bay
- The anesthesia team administers localized blocks, light sedation, or general anesthesia.
- The patient is positioned comfortably on the daycare procedure table.
- The specialized hysteroscope frame is introduced gently through the vagina canal.
- The cervix is carefully accessed without requiring force or deep cuts.
- Sterile saline fluid distends the cavity space, inflating the walls for crisp tracking.
- The specialist thoroughly inspects the lining surfaces to isolate pathologies.
- Targeted micro-tools excise polyps, shave fibroids, or take biopsies before removing the scope.
- Resting quietly under monitoring lines inside the recovery block
- Continuous tracking of blood pressure, heart rates, and respiratory values
- Managing minor cramping signs with basic anti-inflammatory medications
- Detailed post-procedural briefing and discharge paperwork run-through
- Safe same-day discharge to your home once fluids are tolerated comfortably
Before vs After Surgery

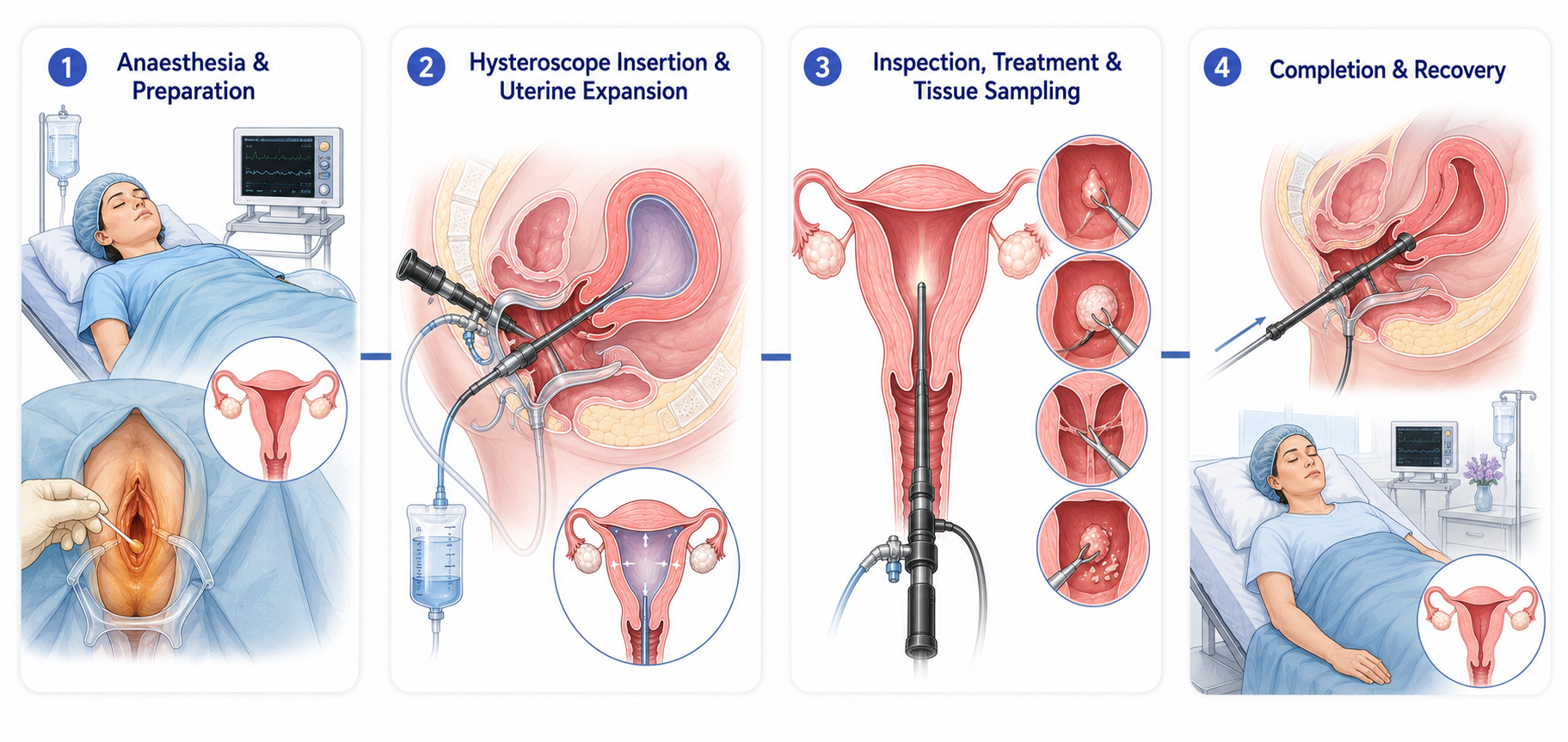
How Is the Surgery Performed?
Step 1
Step 1
Anaesthesia and Preparation
The patient receives anaesthesia or sedation and the vaginal area is cleaned with antiseptic solution.
Patient receives anesthesia or sedation.
Vaginal area is cleaned with antiseptic solution.
Step 2
Step 2
Insertion and Uterine Expansion
The hysteroscope is inserted through the vagina, the cervix is gently accessed, and sterile fluid expands the uterus for better visibility.
Hysteroscope is inserted through the vagina.
The cervix is gently accessed.
Sterile fluid expands the uterus for better visibility.
Step 3
Step 3
Inspection, Treatment and Sampling
The uterine cavity is carefully inspected; polyps, fibroids, scar tissue, or septa may be removed and tissue samples collected if necessary.
The uterine cavity is carefully inspected.
Polyps, fibroids, scar tissue, or septa may be removed if necessary.
Tissue samples may be collected.
Step 4
Step 4
Completion and Recovery
The instruments are removed and the patient is transferred to recovery.
Instruments are removed.
Patient is transferred to recovery.
Duration: Most procedures take approximately 15–60 minutes.
Expert Guidance, Every Step of the Way
Our dedicated care coordinators are here to answer your questions and guide you through every stage of your treatment.
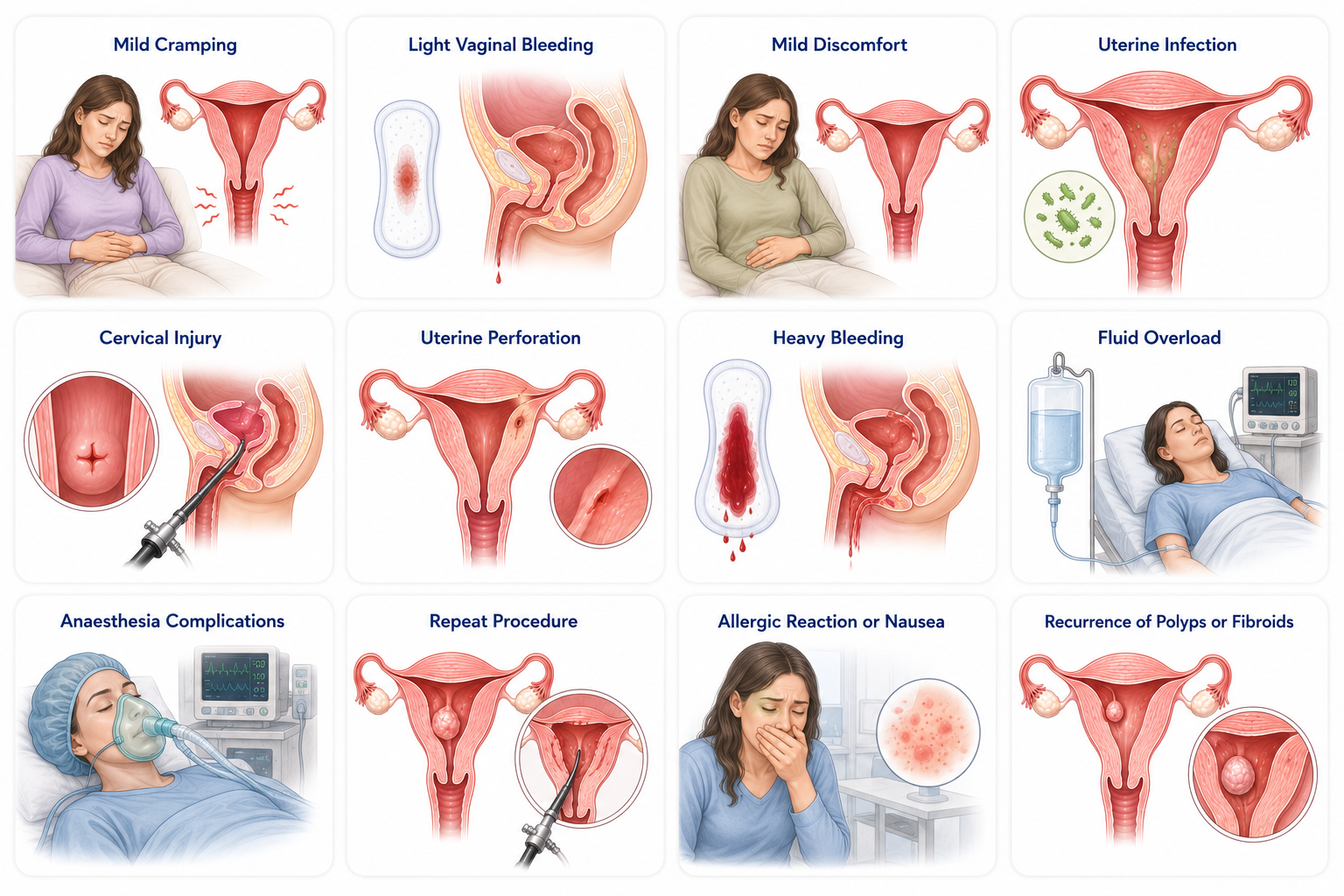
Talk to Our ExpertsPossible Risks and Complications
Like any clinical pelvic intervention, hysteroscopy is highly secure but carries specific manageable risk layers:
1. Common Post-Procedural Realities
- Mild cramps, minor, period-like uterine contractions that settle within a few hours
- Temporary spotting, light vaginal blood discharge or pink tracking lasting a few days
2. Rare Operative Complications
- Uterine perforation, an accidental tiny tear in the thin uterine muscle, typically requiring simple monitoring
- Pelvic infection, microscopic introduction of pathogens into the cavity, safely cleared using targeted antibiotics
- Heavy bleeding, persistent vascular loss from raw tissue beds, managed easily with simple clinical measures
3. Anesthesia Secondary Effects
- Sedation hypersensitivity, mild allergic drug responses or localized skin flares handled instantly by care teams
- Post-op nausea, transient stomach upset or grogginess as sedation compounds leave the bloodstream
Recovery Timeline & Clinical Benchmarks
Postoperative Care Protocols
Inpatient tracking: Post-op care centers around tracking vital sign changes (blood pressure, heart rates), assessing active spot-bleeding, and charting local pain metrics smoothly.
Pain relief: Providing targeted anti-inflammatory drugs and mild analgesics to ensure baseline pelvic comfort before checkout.
Lining recovery rules: Since no open skin wounds exist, focus exclusively on personal genital hygiene and tracking pad absorption rates.
Nutritional guidelines: Resume a balanced, high-protein normal diet gradually, prioritizing hydration and iron-rich choices if pre-op anemia was a factor.
Allowed activity: Light walking and routine administrative tasks are fully secure within 24 to 48 hours of your slot.
Prohibited steps: Avoid heavy weight lifting, sexual intercourse, tampon insertion, or swimming pools until given explicit clearance by your gynaecologist.
Follow-Up Scheduled Reviews
A standard clinical review is typically scheduled 1 to 2 weeks post-procedure. This milestone session ensures the cavity wall is contracting properly, clarifies any bioptic path lab findings, and defines appropriate timelines to safely resume conception planning.
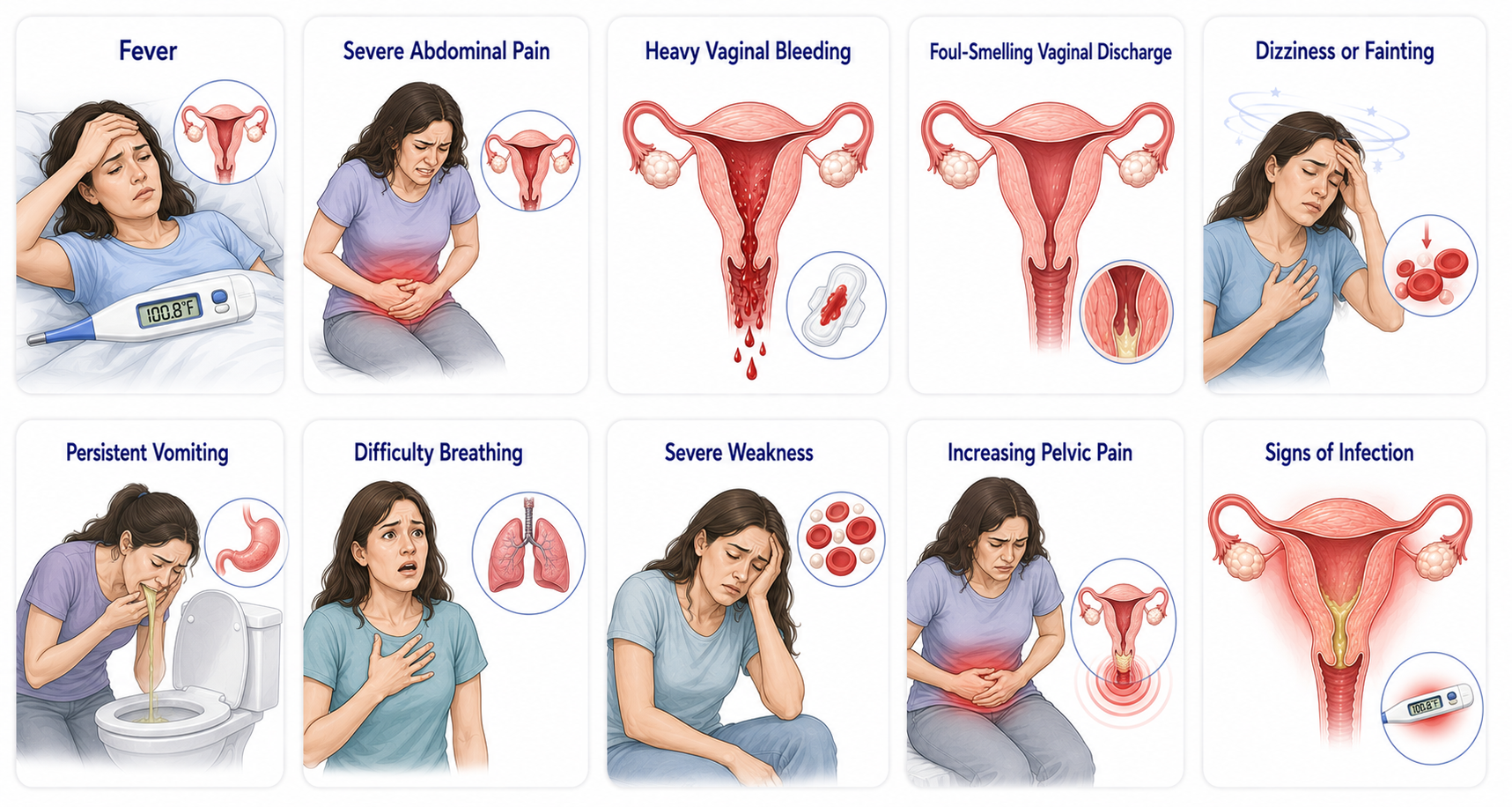
Warning Signs After Surgery
Serious hysteroscopic complications are exceptionally rare. Contact your dedicated care team or present to the emergency room immediately if you note any of these acute indicators:
- Fever spikes developing above 100.4°F (38°C).
- Acute, worsening abdominal cramps or severe deep pelvic pain.
- Heavy bright-red vaginal bleeding that fully saturates a standard sanitary pad within an hour.
- Foul-smelling, thick, or purulent vaginal discharge.
- Sudden waves of dizziness, cold syncopes, or fainting spells.
- Persistent, unresolved vomiting lasting over 24 hours.
- Sudden breathing difficulty, shortness of breath, or sharp chest pain.
Questions to Ask Your Surgeon
- Why do I need hysteroscopy?
- Is this diagnostic or operative hysteroscopy?
- What condition do you suspect?
- Are there alternatives?
- What are the risks in my case?
- Will tissue be sent for biopsy?
- How long will recovery take?
- When can I return to work?
- Will fertility be affected?
- Can this improve my chances of pregnancy?
- What type of anesthesia will be used?
- What symptoms should prompt urgent medical attention?
Frequently Asked Questions
Is hysteroscopy painful?
Most patients experience only mild cramping. Anesthesia or sedation is often used.
Is hysteroscopy a major surgery?
No. It is generally considered a minimally invasive procedure.
Will I need stitches?
No external stitches are usually required.
How long does the procedure take?
Usually 15–60 minutes.
Can I go home the same day?
Yes, most patients are discharged on the same day.
How long will bleeding last?
Light spotting may continue for a few days.
When can I return to work?
Many patients return within 1–3 days.
Can hysteroscopy improve fertility?
It may improve fertility when uterine abnormalities are contributing to infertility.
Can polyps be removed during hysteroscopy?
Yes, polyps are commonly removed during operative hysteroscopy.
Can fibroids be removed during hysteroscopy?
Certain fibroids inside the uterine cavity can be removed.
What is the success rate?
Success rates are generally high when treating appropriate conditions.
Is insurance coverage available?
Many medically necessary procedures are covered.
Can I become pregnant again after hysteroscopy?
Many women can conceive after recovery if fertility factors are favorable.
How soon can I exercise?
Light activity can begin early; strenuous exercise should wait until medical clearance.
When can I travel?
Usually within a few days if recovery is uncomplicated.
Can symptoms return?
Some conditions, such as polyps or fibroids, may recur.
Is anesthesia always required?
Not always. Some office procedures require little or no anesthesia.
What if abnormalities are found?
Treatment may be performed immediately or planned later depending on findings.
Will I have scars?
No external scars are usually created.
How soon can I try for pregnancy?
Your doctor will provide individualized guidance based on the condition treated.
Recent Clinical Studies Redefining Hysteroscopy
Recent international evidence has established hysteroscopy as the gold standard for diagnosing and treating many intrauterine conditions. Contemporary guidelines emphasize office hysteroscopy, minimally invasive operative techniques, and individualized patient selection for managing abnormal uterine bleeding, infertility, recurrent pregnancy loss, retained products of conception, and endometrial pathology. Advances in hysteroscopic technology have also improved procedural safety, patient comfort, and same-day recovery.
Find the Right Specialist
A hysteroscopy is typically performed by a gynecologist, particularly one trained in minimally invasive gynecologic procedures. SPEROW streamlines your patient path by coordinating with elite, high-volume endoscopic consultants across premium daycare structures, ensuring fast healthy recoveries and cashless tracking help.

N V Gowthami Mullangi
VerifiedGynecology
Experience: 15+ Yrs
Hospital: Cygnet Clinics
Languages: Eng
Advanced Surgical Care
Book ConsultationView Profile 
P Farida
VerifiedGynecology
Experience: 10+ Yrs
Hospital: Renova Neelima
Languages: Eng
Advanced Surgical Care
Book ConsultationView Profile 
Reeta Agarwal
VerifiedGynecology
Experience: 23+ Yrs
Hospital: Renova Neelima
Languages: Eng
Advanced Surgical Care
Book ConsultationView Profile
Find a Surgeon You Can Trust
We'll connect you with an experienced specialist who matches your condition, treatment needs, and preferences.
Find the Right SurgeonFree Consultation
FreeGet connected with a trusted doctor for an expert second opinion through our care team.
No Cost Expert Guidance · Coordinated Care · Personalized Support